Immunotherapies are hot property. Immuno-oncology is the crown jewel. But the road to riches, and more importantly cancer cures, is now crowded and full of potholes. Drug hunters need to look ahead, beyond the discovery process itself, to the reality of the many impediments that will confront drug candidates as they proceed towards the clinic in today's landscape. Here, I present three insights from current events, the third one taking a contrarian position.
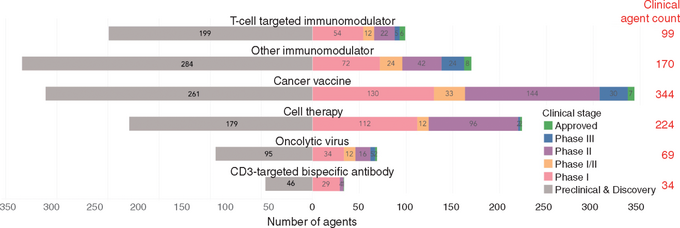
Insight No. 1 is from John Carroll's Endpoints News coverage of the Cancer Research Institute's (CRI) latest "landscape" analysis in the December 2017 Annals of Oncology. There are 2,004 immuno-oncology agents crowding the pipeline, as inventoried in the graphic below. Just in 2017, for example, 469 new PD-1/L1 oncology studies were launched, requiring 52,000 patients to fully enroll them. There are already 164 PD-1/L1 drugs in the works, 50 in the clinic and 5 on the market. These alone have generated over 1,500 trials, before adding in the development burden of 344 cancer vaccines and 224 clinical-stage cell therapies.
The sobering realization from reading these reports is that fanfare surrounding cancer immunotherapy presages an inevitable bust after such a boom. Blame the vagaries of clinical pharmacology, especially the requirements for PK/PD and what is rapidly becoming a structural inability to enroll enough patients. More numbers per trial will be needed to establish at a minimum a dose-response relationship, as well as a broad enough therapeutic index to guarantee safety. And the reality is that there aren't enough patients to go around.
Continue reading
This content available exclusively for BPT Mebmers
We use cookies to personalise content and to analyse our traffic.
You consent to our cookies if you continue to use our website. Read more details in our
cookies policy.